Each year, over 70,000 organs are transplanted worldwide. Unexpected transmission of donor-derived infection is estimated to occur in less than 1% of solid organ transplant recipients, but few data exist that bear directly on the degree of risk of transmission of donor-derived infection through transplantation (41,42). The rate of infection transmission is influenced by a number of factors, including graft type, processing (for many types of tissue allografts), infectious organism and its pathogenicity, donor and recipient characteristics. Immunosuppressed transplant recipients (solid organs, hematopoietic stem cells) have enhanced susceptibility to infections of all types and may act as sentinels for transmissible disease. In addition, signs and symptoms of infection may be modified when compared to typical presentation in the immunocompetent host; this will be influenced by various factors, including the different mechanisms of pathogenesis and host response, and may vary from asymptomatic infection to accelerated, disseminated disease. Diagnosis may be hampered, either due to the lack of immediate, easily recognizable signs and symptoms or failure to suspect the potential origin of infection. In immunosuppressed hosts, the transmission of blood or organ-derived infection due to West Nile Virus, for example, more often manifests as neurological disease with poor clinical outcomes than in normal hosts. Multiple clusters of infection associated with organ transplantation (multiple recipients from the same donor) have included Mycobacterium tuberculosis, Candida and Aspergillus species, herpes simplex virus (HSV), human herpes virus 8 (HHV-8), lymphocytic choriomeningitis virus (LCMV), rabies virus, Trypanosoma cruzi, human immunodeficiency virus (HIV) and hepatitis C virus (HCV).
Detection of these unusual and infrequent transmission events is largely dependent upon the threshold of suspicion of the physicians caring for the transplant recipients; recognition of epidemiologic risk is an influential determinant and once a possible graft-related infection is considered, correct diagnosis will depend on availability of specific pathology specimens, access to appropriate microbiologic and histopathologic advice and testing which might include molecular-based techniques, amongst other things. Prompt reporting of suspicion is vital, enabling centralized and coordinated investigation, with assistance from the appropriate public health or other competent authorities, when and as appropriate.
Infections have also been reported more uncommonly due to tissue transplantation. This lower frequency is likely a reflection of chemical or radiation processing (disinfection) of some tissue grafts including ocular tissue transplants, degree of graft vascularization as well as the normal inflammatory and immune function of the hosts. Some grafts are heavily processed (e.g., bone chips), while some grafts are minimally processed (e.g., cardiovascular tissue). Tissue transplants have been associated with transmission of donor-derived infectious agents, including Candida albicans and other fungi, Elizabethkingia meningoseptica, Clostridium species, rabies virus, HCV, and group A Streptococcus.
Adverse reactions associated with ocular tissue transplantation have been associated with primary graft failures (PGF), bacterial and fungal endophthalmitis and keratitis, corneal dystrophy/degeneration, and scleral graft rejection. Often, although infection is suspected, microbiological cultures may not be obtained routinely and/or a specific pathogen is not identified. A significant reduction in adverse events resulted from use of 5% ophthalmic povidone-iodine solution by eye banks prior to recovery of eyes or corneas.
Haematopoietic stem cells (HPCs) have also been associated uncommonly with transmissions of a wide range of viral (HIV, Parvovirus B19, CMV, EBV, HBV), bacterial (Treponema pallidum, Brucella species, Bacillus species), fungal and parasitic infections (Plasmodium species, Toxoplasma gondii). Transmission of some pathogens, such as bacteria and fungi usually occurs through contamination of the graft rather than being of donor origin.
Table 6. Basic strategies to minimise the risk of infection transmission through transplantation of cells, tissues and organs
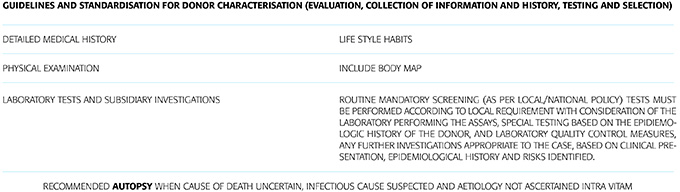
Recommended autopsy when cause of death uncertain, infectious cause suspected and aetiology not ascertained intra vitam
Recommendations:
Response to Possible Allograft-associated Transmission Event
1. The clinician must appropriately consider transmission of infection in association with allograft implantation. Specialist opinion should be sought at an early stage.
2. In the setting of unexpected graft dysfunction, local signs (e.g., erythema, edema, pain) of infection or inflammation, fluid collections or bleeding, recipient samples must be obtained for diagnostic analysis. These may include analysis of both fresh and fixed tissue. Concerning microbiologic methods, Gram stain and culture, bacterial and fungal cultures, and, if appropriate, mycobacterial smears and cultures. Special assays may be indicated based on the nature of the graft or reaction. Complete blood counts with differential counts should also be obtained.
3. Systemic signs of infection or inflammation (fever, leukocytosis, hypotension, confusion, pneumonia, meningismus) merit blood cultures, and sputum or cerebral spinal fluid cell counts, glucose and protein measurement, microbiological cultures and fixed tissue specimens as appropriate to the site of infection and clinical context
4. Donor autopsies should be encouraged when appropriate, and autopsy specimens and other fixed tissue from biopsy should be accessed if there is a transmission investigation.
5. Notification of the organ, eye or tissue bank (as appropriate) of the possibility or demonstration of infection in the allograft donor within 24 hours of re- cognition of potential disease transmission should be made mandatory
6. Notification of the appropriate organizations or public health authorities must be made to ensure appropriate investigation of transmission event.